By Emil Engels, MD, MBA, CPC
VSA President
The Center for Medicare and Medicaid Services (CMS) released two final rules in early November that will impact payment for physician services. On November 2, CMS released the Medicare Physician Fee Schedule Final Rule, which governs payment for physician services beginning January 1, 2018. In addition, CMS published the final Quality Payment Program (QPP) rule that guides participation in MACRA (Medicare Access and Chip Reauthorization Act) via, either the Merit Based Incentive Payment System (MIPS), or Advanced Alternative Payment Models (APMs). CMS usually publishes these final rules around Halloween, and it seems fitting to ask: are they a “trick” or a “treat” for anesthesia providers?
Medicare Physician Fee Schedule Final Rule
CMS publishes a rule annually that “includes updates to payment policies, payment rates, and quality provisions for services furnished under the Medicare Physician Fee Schedule (PFS).” In the proposed rule, CMS lists potentially “misvalued” CPT codes, as required by law. Misvalued CPT codes can be identified in a variety of ways, including looking at increases in utilization, changes in practice expenses, or advances in technology. The anesthesia endoscopy codes were identified as misvalued, which initiated a process of review and solicitation of feedback. Key stakeholders conduct surveys and submit comments, including the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC), the Medicare Payment Advisory Commission (MedPAC), and the American Society of Anesthesiologists (ASA). After considering all comments, CMS decided to create a new set of CPT codes to report anesthesia for endoscopies.
The changes and national utilization data are illustrated in the chart below. Notably, a new code was created for endoscopic retrograde cholangiopancreatography (ERCP) and has a higher base unit value than before. This procedure now has six base units, versus five. On the other hand, reimbursement for lower endoscopies (colonoscopies) has been decreased. Screening colonoscopies will receive only three base units (compared to five previously), and other colonoscopies will have four base units.
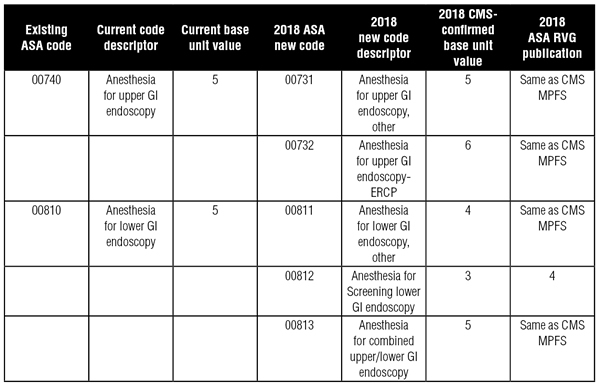 *** NOTE: The term “unit” above refers to the Anesthesia Conversion Factor. To determine the valuation, multiply the number of units by the Anesthesia Conversion Factor.
*** NOTE: The term “unit” above refers to the Anesthesia Conversion Factor. To determine the valuation, multiply the number of units by the Anesthesia Conversion Factor.
The ASA publishes the Relative Value Guide, which assigns values to CPT codes and may govern commercial contracts. The ASA strongly disagreed with CMS’s valuation, and will have a different base value assignment for screening colonoscopies. From the ASA: “The not-so-good news and of interest to many of us is that CMS decreased the base units for screening colonoscopy to 3 base units (00812). ASA strongly disagrees with this decision. Our member survey data supports 4 units, and our Relative Value Guide (RVG) will reflect that. Differing values in the RVG and CMS are not common, but when we strongly disagree and we have survey data to support it, we will be transparent and make the appropriate notations in our RVG.”
In addition, the CPT codes for line placement were identified as potentially misvalued, and new work values were assigned. The changes are summarized in the chart below:
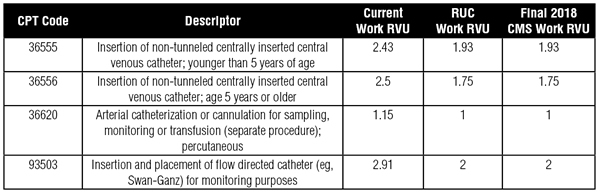 *** NOTE: The term “RVU” above refers to Relative Value Units. To calculate valuation, multiply RVUs by the RBRVS Conversion Factor.
*** NOTE: The term “RVU” above refers to Relative Value Units. To calculate valuation, multiply RVUs by the RBRVS Conversion Factor.
Once again, this change in valuation from CMS is accompanied by a change to the ASA Relative Value Guide (RVG). The values for lines in the RVG will now be listed as “I.C.”, or internal consideration. This means that groups will need to negotiate a rate of reimbursement with commercial carriers.
Medicare Conversion Factors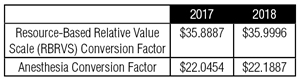
Overall reimbursement to physicians will increase modestly in 2018. The changes are summarized in the table at right.
Percutaneous Implantation of Neurostimulator Arrays
Another piece of good news for chronic pain physicians – CMS significantly increased the work valuation for percutaneous implantation of neurostimulator arrays. CPT codes 64453 (percutaneous implantation of neurostimulator electrode array; cranial nerve) and 64555 (percutaneous implantation of neurostimulator electrode array; peripheral nerve) were revalued upward approximately 250%.
Changes to the Value-Based Payment Modifier in 2018
The 2018 payment year, based on 2016 performance, will be the final year of the value-based payment modifier (VM). Providers will receive an upward or downward adjustment to their payments based on how well they performed in 2016. In the final rule, CMS made several allowances to align the program more with MACRA and ease the reporting burden for providers. First, providers need only report six quality measures for 2016, in contrast to the original requirement of nine. In addition, CMS will be agnostic to the National Quality Strategy (NQS) domain of those measures and is waiving the requirement for a cross-cutting measure. Finally, CMS has eased the downward adjustments under the VM, much like the “Pick Your Pace” program for MACRA. Those who successfully submit data will avoid a downward adjustment from quality tiering. CMS is also reducing the penalties for those groups who did not participate in PQRS from 4% to 2% (for groups of 9 or less, the penalty goes from 2% to 1%).
MACRA and MIPS in 2018
In my November 2, 2017 article in Anesthesiology News entitled “MACRA 2018: A Look Ahead,” I discuss changes to the Quality Payment Program in 2018. That guidance was based on the proposed rule, and since that time, the final rule including additional significant changes has been published. These changes to the MIPS program are summarized below.
Quality Reporting
The data completeness threshold has been increased from the proposed rule. In the proposed rule, the threshold was set at 50%, but it has been increased to 60% in the final rule. This means that you must submit quality data on 60% of eligible patients for a particular measure (including commercial insurance) in 2018. The margin for error is getting smaller, so it will be important to have effective quality data capturing and reporting early in the year.
In addition, the final scoring threshold has been set at 15 points. A full discussion of scoring is beyond the scope of this article, but a provider must score at or above the threshold to avoid a penalty. In 2017, the threshold was 3 points, and a provider could avoid a penalty by submitting one measure, one time, for one patient. In 2018, clinicians need to submit multiple measures and should participate in the improvement activities category to avoid a penalty.
Cost
The cost category was originally proposed to have zero weight. However, in the final rule, cost has been assigned a weight of 10%. No action is required on your part – cost data is collected on an administrative basis from claims. However, you should be aware of how the cost score is calculated. In order to be held accountable for cost, your practice has to be attributed patients. Most anesthesia providers will not be attributed patients. If you are attributed patients, CMS will be looking at two cost measures continued from the value-based modifier: Total Costs Per Capita and Medicare Spending Per Beneficiary. In the future, CMS will include costs related to episodes of care, like surgeries, and anesthesiologists will have greater exposure in the cost category.
2018 Score Weighting
As I described in the November 2017 article, most anesthesia providers will be excluded from the advancing care information category. If you have attributed patients, the cost category will count 10% towards your final score. In this situation, your final score will be weighted as follows: 75% quality, 10% cost, and 15% improvement activities. If you don’t have attributed patients, cost will not count, and your final score will be weighted 85% quality and 15% improvement activities.
Exemption for Extreme and Uncontrollable Circumstances
CMS acknowledges that many clinicians have been impacted by recent natural disasters, including hurricanes Harvey, Irma, and Maria. Natural disasters and other uncontrollable circumstances impede a physician’s participation in the Quality Payment Program. CMS provides examples of uncontrollable circumstances, including a hurricane, natural disaster, or public health emergency. Clinicians can apply for an exemption, and those in affected areas will receive an automatic exemption. To quote CMS: “Clinicians in affected areas that do not submit data will not have a negative adjustment. We know that the circumstances have created a significant hardship that has affected the availability and applicability of measures.”1 However, if you live in an affected area and submit data, you will be scored: “Clinicians that do submit data will be scored on their submitted data. This allows them to be rewarded for their performance in MIPS. Because MIPS is a composite, clinicians have to submit data on two or more performance categories to get a positive payment adjustment.”1 For more information, please visit the QPP website: qpp.cms.gov.
Conclusion
Healthcare is changing at a rapid pace, as evidenced by the two final rules released in November. To be successful, clinicians must keep pace and adjust to the ever changing reimbursement landscape. Anesthesia providers had payments for colonoscopies and line placement reduced, while reimbursement for implantation of neurostimulators and the conversion factor increased. The Quality Payment Program moves ahead, with several key changes that continue the shift from paying for volume to value. The author and Anesthesiology News will endeavor to keep readers informed about important quality and payment issues in the future.
Look for future columns on other quality reporting topics.
Dr. Engels is a Division Medical Officer with MEDNAX and can be reached at [email protected].
This column includes information from the Centers for Medicare & Medicaid Services (CMS) and represents the author’s best interpretation of available resources. The author is not recommending specific methods for participating in MACRA. Providers who have questions should consult a compliance professional or contact the CMS Quality Payment Program Help Desk by sending an email to [email protected].
References
- Quality Payment Program Year 2 Final Rule Overview, found at cms.gov.